High Flow Oxygen Therapy (HFOT)
High Flow Oxygen Therapy (HFOT)
High flow Oxygen therapy delivered through AquaNASE® nasal cannula heats and humidifies the gases with flows
Applications
High Flow – Oxygen therapy delivered through AquaNASE® nasal cannula heats and humidifies the gases with flows up to 60 L/min, reducing oxygen dilution.
- Improved patient comfort
- Reduced oxygen dilution
- Dead space washout
- Improved secretion clearance
- Alveoli recruitment
CPAP – Continuous Positive Airway Pressure (CPAP) is delivered to correct hypoxia. Indications include cardiogenic pulmonary oedema and atelectasis.
CPAP recruits collapsed alveoli and improves gas exchange by:
- Application of PEEP (Positive End Expiratory Pressure) valve to maintain expiratory pressure.
- Delivering flow to meet the patients peak inspiratory requirements and maintain PAP.
- Delivery of CPAP is confirmed via pressure manometer.

AquaNASE®
AquaNASE® cannula for HFHOT can be supplied with AquaVENT® breathing systems in a complete Flowkit.
Patients can eat, drink, communicate and mobilise pulmonary secretions without disrupting therapy support. Heated humidification helps prevent drying of upper airway mucosa increasing patient comfort during oxygen therapy. Flows closer to a patient’s inspiratory demand reduces ambient air entrainment and oxygen dilution.
Use AquaNASE® during patients non-invasive ventilation rest periods for:
- oral hygiene
- hydration
- feeding
- physiotherapy
- managed weaning


High Flow Oxygen Therapy Video
POINT plus CPAP
PEEP versus CPAP; what’s the difference?PEEP & CPAP are often mistaken as one and the same therapy. Defining the difference helps us understand the benefits and limitations of each therapy.
POINT Plus (CPAP)
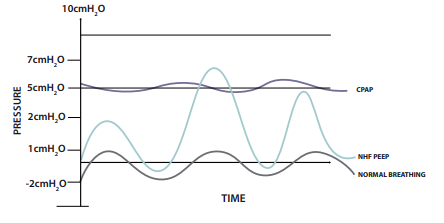
- PAP is any pressure applied to the airways above atmospheric pressure.
- PEEP refers to the positive airway pressure at the end of expiration only. During inspiration the pressure will drop below the PEEP level.
- CPAP refers to the PEEP pressure being maintained during the entire respiratory cycle (inspiration and expiration).
- To prevent a drop of pressure during the respiratory cycle the flow rate must exceed the patient’s peak inspiratory flow rate. In respiratory distress PIR may range from 60-120L/min